

Scrub typhus is a bacterial infection caused by Orientia tsutsugamushi – an organism that lives and multiplies exclusively inside human cells, It spreads through the bite of an infected larval mite – commonly called the scrub typhus insect or chigger.
This is not a disease passed between people. One mite, one bite, and the bacteria enters your bloodstream.
The disease is endemic across South and Southeast Asia. In India, states like Himachal Pradesh, Uttarakhand, Sikkim, Tamil Nadu, and the Northeast report the highest case loads — particularly between July and November, peaking during and after the monsoon season.
According to a 2024 multicentric study published in PLOS Neglected Tropical Diseases, an estimated one million cases occur globally each year, with India contributing a disproportionately high share due to underreporting and frequent misdiagnosis as dengue or typhoid.
The entry point is always the same: a bite from an infected insect to a human host.
Read: Main Cause of Scrub Typhus
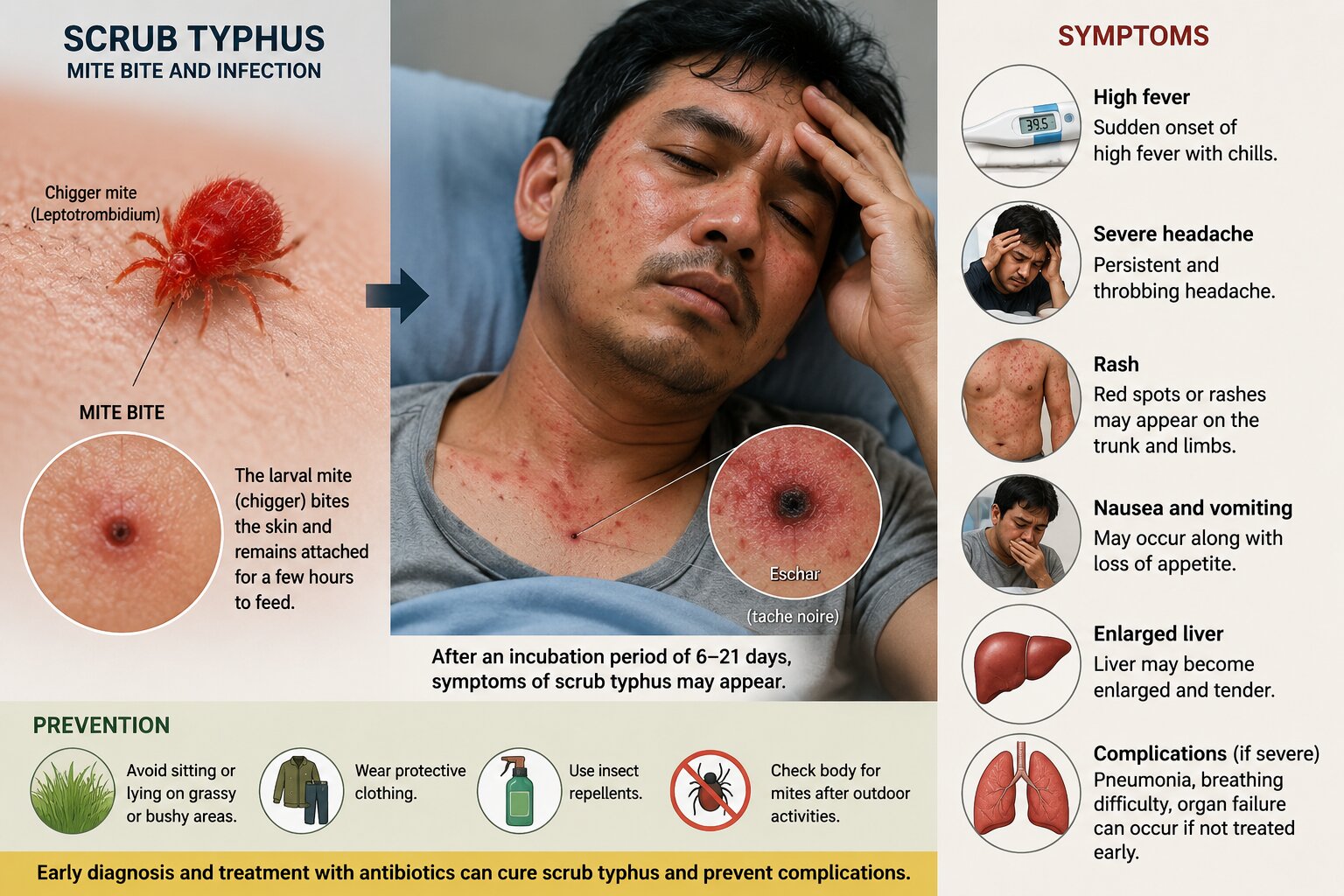
What Happens When a Chigger Mite Bites a Human?
When a chigger mite bites, it injects Orientia tsutsugamushi directly into the skin – and in most cases, you will not feel it happen.
The larval mite (Leptotrombidium species) is 0.2 mm in size – invisible without magnification. It targets warm, hidden body areas: armpits, groin, waistband, behind the knee, and the hairline. It does not burrow. It attaches to a skin pore, feeds for 2 to 3 days, and falls off — leaving behind the bacteria and a small, painless dark-crusted ulcer called an eschar.
The eschar is the most diagnostically important sign of scrub typhus. It appears in approximately 50 to 70% of patients, but is frequently missed because it hides in skin folds or under hair.
From the bite site, bacteria enter the lymphatic system and then the bloodstream – targeting the cells lining your blood vessels. This vascular damage is what drives multi-organ complications in untreated cases.
Incubation period: 6 to 21 days. Symptoms appear long after the mite has gone, which is why most patients have no memory of being bitten.
Read: Type of Fever in Scrub Typhus
Symptoms of Scrub Typhus
Scrub typhus begins with sudden high fever, severe headache, and body pain nearly identical to dengue. The key clinical clue that separates it is the eschar and a trunk-first skin rash that follows within the first week.
Days 1 to 5:
- Fever: 102 to 104 degrees F, continuous
- Severe frontal headache
- Generalised muscle ache and fatigue
- Chills, loss of appetite
- Eschar at the bite site (painless dark scab – check hidden skin areas)
Days 6 to 10:
- Maculopapular rash — starts on the trunk, spreads outward
- Swollen lymph nodes near the eschar
- Mild cough, red eyes
Beyond Day 10 — Seek Emergency Care Immediately If:
- Confusion or disorientation
- Breathlessness
- Reduced urine output
- Jaundice
- Chest pain or irregular heartbeat
A 2023 hospital study from AIIMS Rishikesh found that 68% of scrub typhus patients presenting with complications had already received treatment for viral fever or dengue for 5 or more days before the correct diagnosis was made.
Read: Symptoms of Scrub Typhus in Detail
Risk Factors of Scrub Typhus
Your risk of scrub typhus is almost entirely determined by where you spend time — not who you are.
Chigger mites thrive in the transition zone between soil and vegetation: tall grass, leaf litter, forest edges, riverbanks, and agricultural fields.
High-risk environments:
- Paddy fields and agricultural land during monsoon and post-monsoon months
- Forested trekking routes and jungle clearings
- Riverbanks and stream-side vegetation
- Overgrown plots near residential areas – a 2024 surveillance report identified peri-urban scrub typhus as a growing pattern in construction-adjacent zones in South India
- Himalayan pilgrimage and trekking routes (July to October)
What specifically to avoid:
- Sitting or resting directly on grass or soil in endemic areas
- Walking through dense vegetation in open footwear
- Leaving shirt untucked — the waistband is a primary mite attachment zone
- Drying clothes on grass in rural areas
Prevention of Scrub Typhus
Scrub typhus prevention is 100% behavioural — there is no approved vaccine yet. The right clothing, repellents, and a post-exposure body check are your only defences.
Before entering a risk area:
- Apply DEET-based repellent (20% or above) on all exposed skin
- Treat clothing with permethrin — focus on sock tops, trouser hems, and cuffs
- Wear full sleeves, long trousers tucked into socks, and closed footwear
During outdoor activity:
- Use a ground mat — never sit directly on grass or soil
- Stay on cleared paths where possible
After returning home — The 3-Step Check:
- Shower within 2 hours
- Do a full-body skin scan: armpits, groin, hairline, behind ears, waistband. Look for a small painless dark scab
- Machine-wash clothes at high heat
Scrub TyphusVaccine Update (2025): The Oxford START Trial is currently evaluating a scrub typhus vaccine in adults across endemic Asian regions, with early-phase immunogenicity data showing a measurable antibody response. The extreme genetic diversity of Orientia tsutsugamushi strains remains the primary challenge. A licensed public vaccine is still several years away.
Treatment for Scrub Typhus
Scrub typhus is fully curable. Doxycycline started within the first 5 days brings fever down within 24 to 48 hours. The problem is not the disease; it is the diagnostic delay.
First-line treatment:
- Doxycycline 100 mg — twice daily, oral, for 7 to 14 days depending on severity.
Alternative — Azithromycin:
- Preferred for children under 8, pregnant women, and doxycycline-intolerant patients
- The INTREST Trial (2023, NEJM) confirmed azithromycin is non-inferior to doxycycline in uncomplicated scrub typhus
Emerging Concern — Antibiotic Resistance: Doxycycline-resistant strains, first confirmed in South Korea, have been reported in isolated cases from Northeast India (2024). Rifampicin is used in these cases and in severe multi-organ presentations.
Scrub Typhus Severity and Treatment – Quick Reference:
| Severity | Key Features | Treatment | Duration | Setting |
| Mild | Fever + eschar only | Doxycycline 100mg BD oral | 7 days | Outpatient |
| Moderate | Rash + lymph nodes + mild LFT rise | Doxycycline oral | 10 to 14 days | Outpatient with monitoring |
| Severe | Lung, kidney, or liver involvement | IV Doxycycline or IV Azithromycin | 14 to 21 days | Inpatient |
| CNS / Critical | Encephalitis, organ failure | IV Doxycycline + Chloramphenicol | 21 days | ICU |
| Paediatric / Pregnant | Any severity | Azithromycin oral or IV | 5 to 7 days | As per severity |
Recovery from Scrub Typhus
With timely treatment, most patients recover fully within 2 weeks. Complicated cases take longer, and a small subset experience lingering symptoms.
Typical Recovery Timeline:
- Day 1 to 2 post-treatment: Fever begins to break — the clearest early sign the antibiotic is working
- Day 3 to 5: Fever resolves. Headache and body pain ease progressively
- Week 2: Most patients resume normal activity. Liver enzymes and platelet counts normalise
- Week 3 to 6: Full energy restoration in moderate cases. Severe cases may take 6 to 8 weeks
Post-Scrub Typhus Syndrome: A 2024 follow-up study from South India found that 17% of recovered patients reported persistent fatigue, difficulty concentrating, and weakness beyond 6 weeks post-discharge – a pattern researchers now call post-scrub typhus syndrome.
Can It Come Back? Yes. Orientia tsutsugamushi has multiple genetically distinct strains. Recovery from one strain does not protect against another. People in endemic areas remain at risk of re-infection in future seasons.
Follow-Up Recommended:
- Liver function test at 2 weeks post-treatment
- Platelet count recheck if initially low
- Report any new fever within 3 months to your treating doctor immediately
About Author : Dr. Kunal Behal (Consultant – General Medicine) for public awareness. It does not replace medical consultation. If you suspect scrub typhus, seek evaluation from a qualified physician without delay.
To Book an Appointmeent: Click Here



