Written By Dr Neelakanth Parappanavar Consultant Gastro, Liver & Endoscopy At Amcare Hospital Zirakpur.
Hepatitis A is an acute, highly contagious liver infection caused by the Hepatitis A virus (HAV), which is a single-stranded RNA virus belonging to the Picornaviridae family. Unlike other types of viral hepatitis, Hepatitis A does not cause chronic liver disease.
It is, in most cases, a self-limiting illness, meaning the immune system resolves the infection without antiviral medication. However, in vulnerable populations like the elderly, immunocompromised individuals, and those with pre-existing chronic liver diseases , it can trigger acute liver failure, which is life-threatening.
Globally, the World Health Organization estimates approximately 1.4 million clinical cases of Hepatitis A annually, though the true number is believed to be several times higher due to unreported mild cases. It remains one of the most common vaccine-preventable liver diseases worldwide.
As a practicing gastroenterologist, I want to emphasize something often misunderstood: Hepatitis A is not the same as Hepatitis B or C. It belongs to a distinct group among the types of viral hepatitis, and its transmission, treatment, and long-term outcomes differ significantly.
What Causes Hepatitis A?
The Hepatitis A virus is the sole causative agent of this infection. The virus primarily targets hepatocytes , the liver’s functional cells and replicates within them, triggering an immune-mediated inflammatory response that causes the characteristic liver injury seen in patients.
The virus is extraordinarily resilient in the environment. It can survive on surfaces for several hours, in water for months, and withstands freezing temperatures. This biological hardiness is a major reason outbreaks are difficult to contain once they begin, particularly in areas with inadequate sanitation infrastructure.
Key risk factors that predispose individuals to HAV infection include:
- Living in or traveling to high-endemicity regions (parts of South Asia, sub-Saharan Africa, Central America).
- Consumption of contaminated food or water – particularly raw shellfish, unwashed produce, and ice from untreated sources.
- Close contact with an infected person, especially within households.
- Men who have sex with men (MSM) – a clinically recognized high-risk group, consistent with CDC and WHO epidemiological data.
- People who use injectable or non-injectable drugs.
- Individuals experiencing homelessness or living in overcrowded conditions.
- Immunocompromised individuals and those with existing chronic liver diseases such as cirrhosis or hepatitis B or C co-infection.
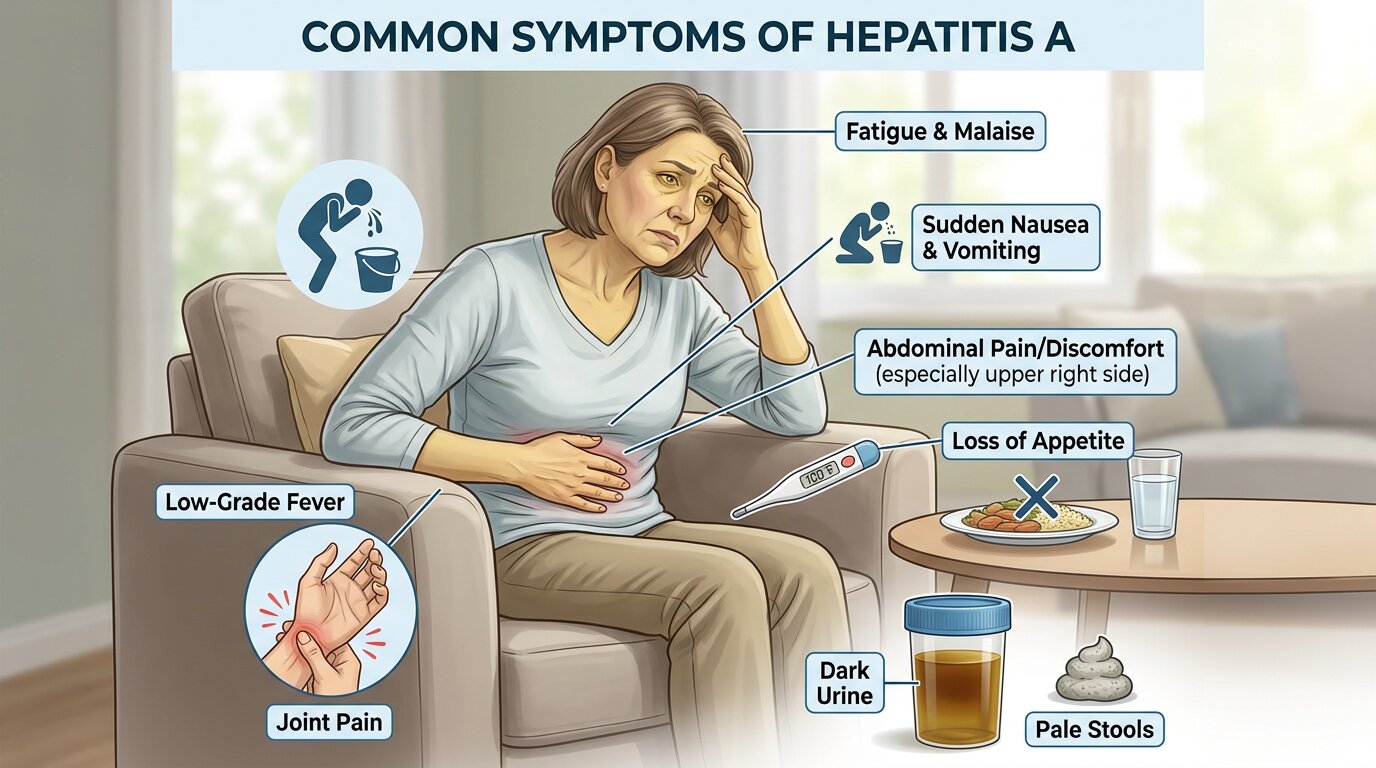
Symptoms of Hepatitis A
One of the most clinically significant features of Hepatitis A is the spectrum of disease severity , from entirely asymptomatic infection to fulminant hepatic failure.
In children under 6, up to 70% of infections are asymptomatic, which contributes silently to community spread. Adults, by contrast, are far more likely to develop symptomatic disease, and their illness tends to be more severe.
The incubation period for Hepatitis A is typically 15 to 50 days (average: 28 days) – the window between viral exposure and symptom onset.
Early Symptoms (Prodromal Phase- Days 1 to 7):
- Fatigue and malaise
- Nausea and vomiting
- Loss of appetite (anorexia)
- Low-grade fever (38–39°C)
- Abdominal discomfort, particularly in the right upper quadrant (over the liver)
- Myalgia (muscle aches) and headache
Icteric Phase (Days 7 Onward – When Liver Involvement Becomes Visible):
- Jaundice – yellowing of the skin and whites of the eyes (scleral icterus)
- Dark urine (bilirubinuria) – often described as “cola-colored”
- Pale or clay-colored stools
- Pruritus (intense itching caused by bile salt deposition in skin)
- Hepatomegaly – a palpably enlarged, tender liver on clinical examination
When to Seek Immediate Medical Attention:
If a patient presents with progressive jaundice, confusion, coagulopathy (easy bruising/bleeding), or severe abdominal pain, this must be treated as a potential acute liver failure emergency. In clinical practice, I’ve seen cases , particularly in patients over 50 with underlying liver disease escalate rapidly. Early hospitalization saves lives.
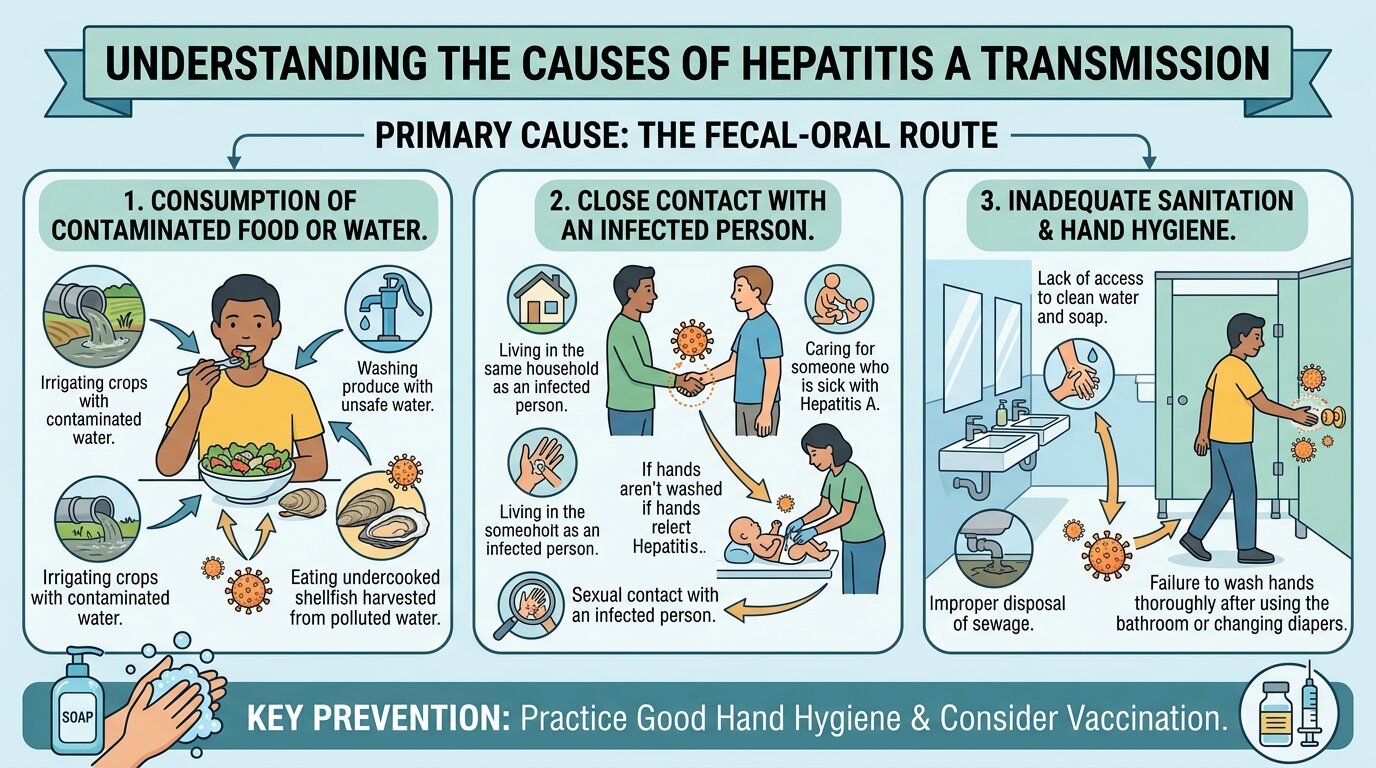
How Is Hepatitis A Transmitted?
Hepatitis A spreads almost exclusively through the fecal-oral route , which means that the virus is shed in the feces of infected individuals and enters a new host via ingestion.
Primary Transmission Pathways:
1. Contaminated Food and Water: This is the most common global transmission route. Foods implicated include raw or undercooked shellfish (clams, oysters, mussels) harvested from polluted waters, raw vegetables fertilized with human waste, and untreated drinking water. Food handlers who are infected and practice poor hygiene can contaminate entire food batches before they show symptoms.
2. Person-to-Person Transmission: Direct contact with an infected person , particularly household members, sexual partners, and caregivers carries significant transmission risk. HAV is present in stool from approximately 2 weeks before symptom onset through 1 week after jaundice appears, meaning infected individuals are most contagious before they even know they’re ill.
3. Sexual Transmission: Oro-anal sexual contact is a documented transmission route, which is why men who have sex with men represent a high-risk demographic. Several large urban outbreaks in recent years have been traced to sexual contact networks.
4. Contaminated Surfaces and Objects: HAV can survive on hands, utensils, and surfaces for extended periods. Shared needles among people who inject drugs also facilitate transmission, though this is secondary to fecal-oral spread.
Importantly: Hepatitis A is NOT transmitted through blood transfusions, coughing, sneezing, or casual contact such as sitting next to an infected person. This distinguishes it from Hepatitis B and C, which are primarily bloodborne.
Is Hepatitis A Curable?
Yes – Hepatitis A is curable. This is a key distinction that patients must understand.
Unlike Hepatitis B (which can become chronic in adults ~5% of the time) or Hepatitis C (which becomes chronic in ~75–85% of cases), Hepatitis A does not establish chronic infection.
Once the immune system successfully clears the virus , which it does in virtually all immunocompetent patients , the liver heals completely, leaving no lasting damage and no carrier state.
Furthermore, recovery from Hepatitis A infection confers lifelong immunity to the virus. Once you’ve had it, you cannot get it again.
The exception and I cannot stress this enough clinically is the rare occurrence of fulminant hepatic failure, which occurs in less than 1% of cases overall but rises to nearly 1.8% in patients over 50 and significantly higher in those with underlying chronic liver diseases such as cirrhosis or chronic Hepatitis B or C co-infection. These cases require urgent management in a liver specialty center, and liver transplantation may become the only life-saving option.
How to Treat Hepatitis A
There is no specific antiviral treatment for Hepatitis A. The cornerstone of management is supportive care , a treatment philosophy grounded in the understanding that the healthy immune system, given the right conditions, will eliminate the virus.
Standard Supportive Treatment Protocol:
1. Rest : Physical rest is essential, particularly during the acute phase. Fatigue in Hepatitis A can be debilitating, and forcing activity worsens recovery. I advise complete activity restriction until liver enzyme levels normalize on serial blood tests.
2. Hydration and Nutrition: Nausea and vomiting can impair oral intake significantly. Patients must maintain adequate hydration. Small, frequent, low-fat, high-carbohydrate meals are best tolerated. In hospitalized patients, IV fluids and antiemetics are administered as needed.
3. Avoid Hepatotoxic Agents – Absolutely No Alcohol: The liver is under enormous stress during active HAV infection. Alcohol must be completely eliminated for the duration of illness and for at least 6 months after recovery. NSAIDs like ibuprofen and naproxen should be avoided. Acetaminophen (paracetamol) should only be used at minimum doses if absolutely necessary.
4. Medication Review : Many prescription medications are hepatically metabolized. Dosing adjustments may be required. Always inform your gastroenterologist of all medications, supplements, and herbal products being taken.
5. Monitoring via Blood Tests: Regular liver function tests (LFTs) – including ALT, AST, bilirubin, and prothrombin time (PT/INR) – are essential to monitor disease trajectory. A blood test confirming anti-HAV IgM antibodies is how Hepatitis A is definitively diagnosed. Rising INR or falling albumin signal deteriorating liver synthetic function and require urgent escalation of care.
6. Hospitalization Criteria: Patients requiring hospital admission include those with: inability to maintain oral intake, INR ≥ 1.5, encephalopathy, severe jaundice with bilirubin > 10 mg/dL, or any signs of acute liver failure.
Recovery From Hepatitis A:
Most patients recover fully within 2 months. However, a subset – approximately 10–15% – experience a relapsing course, where symptoms temporarily improve then return weeks later. This relapse is self-limiting and does not indicate chronic infection or worse prognosis. Complete recovery, even in relapsing cases, is the expected outcome.
Liver enzyme normalization on blood tests is the objective marker of full hepatic recovery.

How to Prevent Hepatitis A
Prevention is, without question, the most effective strategy against Hepatitis A and the tools we have are excellent.
1. Hepatitis A Vaccine -The Most Powerful Preventive Tool
The Hepatitis A vaccine is safe, highly effective, and provides long-term , likely lifelong protection. It is administered as a two-dose series, with the second dose given 6 to 12 months after the first.
Who should receive the Hepatitis A vaccine?
- All children at age 1 (routine childhood immunization in many countries)
- Travelers to endemic regions
- Men who have sex with men
- People with hepatitis B or C or any chronic liver disease
- People who use drugs (injectable or non-injectable)
- Household contacts of adopted children from endemic countries
- Anyone without documented prior immunity who wants protection
A combined Hepatitis A and B vaccine is also available (Twinrix), which is particularly valuable for travelers and individuals with multiple risk factors.
2. Rigorous Hand Hygiene
Handwashing with soap and water for at least 20 seconds after using the bathroom, changing diapers, and before handling food is the single most impactful non-vaccine preventive measure. Alcohol-based hand sanitizers are not reliably effective against HAV – soap and water is the standard.
3. Safe Food and Water Practices
- Drink bottled or boiled water in high-risk regions
- Avoid raw shellfish unless sourced from certified, clean waters
- Wash all fruits and vegetables thoroughly before consumption
- Avoid raw produce from unknown sources in endemic areas
- Avoid ice in countries with questionable water treatment systems
4. Safe Sexual Practices
Using barrier protection (dental dams, condoms) during oro-anal contact reduces transmission risk among sexual contacts.
5. Outbreak Response and Public Health
When a Hepatitis A case is identified, close contacts should receive post-exposure prophylaxis immediately. Public health authorities must be notified to identify common-source outbreaks, particularly those linked to contaminated food.
Final Clinical Perspective
Hepatitis A, while self-limiting in the vast majority of cases, should never be dismissed as a minor illness. In the right host like elderly, immunocompromised, or with existing chronic liver diseases , it can be fatal. The Hepatitis A vaccine remains one of medicine’s most elegant public health tools: safe, effective, and capable of preventing a disease with no specific cure.
As a gastroenterologist, my advice is unambiguous: vaccinate if you haven’t already, practice strict hand hygiene, and seek early medical evaluation if you develop jaundice, dark urine, or significant fatigue after potential exposure. A simple blood test can confirm or rule out the diagnosis within hours, and early monitoring ensures that the rare severe case is caught before it becomes a crisis.
Hepatitis A is curable , but prevention is always better than treatment.